

COVID-19と心血管系疾患 COVID-19 and Cardiovascular Diseases:Latest Updates
COVID-19は、2020年5月現在もなお、世界中で猛威を振るっています。COVID-19に関する世界中の研究報告が蓄積されているなかで、心血管系疾患は予後と関連することもあり、注目されています。以前のコラム >でもとりあげましたが、さらにCOVID-19と心血管系疾患についてのアップデートとして、ヨーロッパ心臓病学会のガイダンスらの最新の報告をもとに概説します。
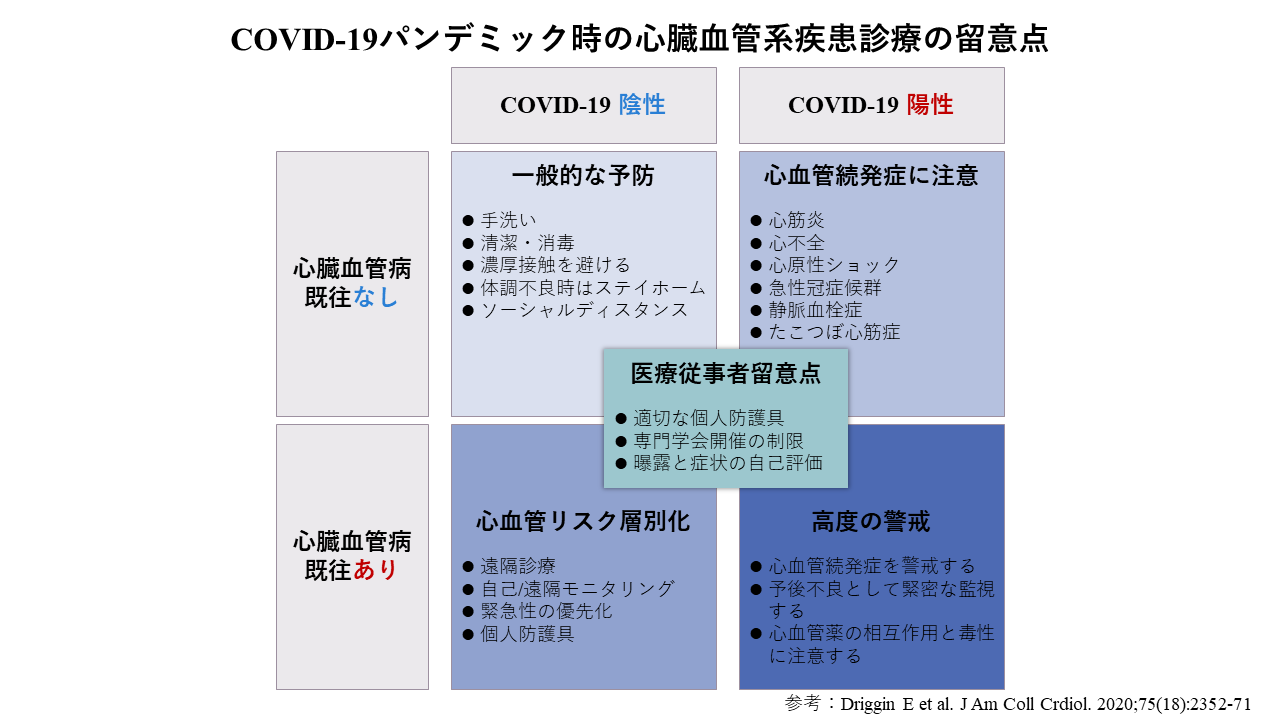
COVID-19と心血管系疾患
COVID-19と心血管系疾患についてのヨーロッパ心臓病学会ガイダンスにおいても、心血管疾患を有していることが、COVID-19の重症化および死亡のリスクになる可能性が高いとしています(文献1)。また、NEJMに報告されている国際登録データベースを用いた8,910例の検討では、基礎疾患に心血管疾患を有することが、COVID-19感染症患者の院内死亡のリスク上昇に関わると報告しています(文献2)。COVID-19感染症の重症化と心血管疾患の関係は明らかになりつつあります。ただし、高齢であることが、重症化や死亡に強く影響するため、交絡バイアスの見極めは重要です。
また、COVID-19感染により続発する心血管疾患として、トロポニン上昇でサロゲートされる心筋障害もガイダンスで取り上げられています。COVID-19感染症による入院患者1,004例を対象とする心筋トロポニンで定義した心筋障害と死亡率との関連を解析した中国の単施設コホート観察研究では、トロポニンが高い群では、人工呼吸器管理になる重症例が多く、また死亡率も有意に高かったと報告されています(文献3)。そしてCirculationの最新レビューからは、心筋障害はCOVID-19感染症の約4分の1に存在し、発症時に急性の心筋障害を呈するものと、全身状態の悪化に伴って進行する心筋障害という2つのパターンで発現するとまとめています(文献4)。
COVID-19とACE阻害薬・ARB
欧米のガイダンスでもCOVID-19とレニン・アンギオテンシン系酵素であるACE2の関連の問題が取り上げられています(文献1, 文献5)。SARS-CoV2はACE2受容体を介して細胞に侵襲します。ACE阻害薬・ARBはACE2を増加させるという基礎研究報告があるため、SARS-CoV2感染感受性を増加させるという仮説があります。しかし、現時点で、ACE阻害薬やARB治療とSARS-CoV2感染に対する感受性や、経過との間の関連性における臨床的エビデンスは示されていません。欧米のガイダンスにおいてもACE阻害薬・ARBの中断は原疾患増悪のリスクがあり、現時点においては、COVID-19感染に関わらず継続すべきであると推奨しています。
NEJMに掲載された国際登録データベースを用いた8,910例の検討では、臨床背景でのACE阻害薬・ ARB服薬とCOVID-19感染症患者の院内死亡との有害な関連の可能性は確認されなかったと報告されています(文献2)。また、イタリアからの大規模な住民ベースの研究では、ACE阻害薬・ARBがCOVID-19リスクに影響を及ぼすというエビデンスは認められなかったと報告しています(文献6)。現状においては、COVID-19感染症とACE阻害薬・ARBの関連性を示唆するエビデンスはなく、これらの心血管系疾患治療薬を中断することによるデメリットのほうが大きいと考えられ、内服の継続が推奨されています。
COVID-19と血栓症
COVID-19感染患者に若年の脳梗塞などの血栓症が報告されるようになり、COVID-19と血栓症の関連が注目されています。厚生労働省からの「新型コロナウイルス感染症(COVID-19)診療の手引き 第2版」においても、重症度分類とマネージメントのトピックスに血栓症対策が取り上げられています(文献7)。重症感染症や重症肺炎が、深部静脈血栓症(DVT)の中等度リスクである背景に加え、COVID-19感染症患者では、サイトカインストームや血管内皮障害などにより、線溶系の異常が起き、Dダイマーが正常上限を超える場合には、ヘパリンなどの抗凝固療法実施を推奨しています。実際に、COVID-19感染確定患者191例を対象とする院内死亡のリスク因子を解析した2施設コホート観察研究では、入院時のDダイマーが1.0μg/ml以上の上昇は院内死亡のリスク因子と報告しています(文献8)。
また、COVID-19感染症による入院患者143例を対象とするDVTの発症率、DVT合併の予後などを解析した単施設コホート観察研究では、下肢静脈超音波検査により診断されるDVTは66名(46%)と約半数に認められ、DVT発症群とDVT非発症群の死亡率を比較するとDVT発症群は有意に死亡率が高いと報告しています(文献9)。さらに、JACCのResearch Lettersからは5施設に入院したCOVID-19確定患者2,773例を対象としたコホート研究において、抗凝固療法実施(経口, 皮下注射, 静脈注射)と生存との関連を評価し、抗凝固療法実施群(786例)では、非実施群に比べて院内死亡率は僅かに低い程度であるが(実施群22.5% 対 非実施群22.8%)、生存期間が長いこと(中央値21日 対 14日)が示されています(文献10)。
このように、COVID-19と血栓症の関連性は強いという証拠が出始め、抗凝固療法の推奨もされるようになってきていますが、抗凝固療法には出血という大きな合併症があります。COVID-19症例における抗凝固療法の適応については、その適応と出血合併症に注意しながら、更なるガイダンスの発表が待たれます。
With CORONAの時代をむかえ、CORONAで命を落とさないために、日頃から心血管系疾患を管理することが重要であり、そしてたとえ目の前の患者さんがCORONAに罹患していたとしても、二次性心筋障害のリスクのためのトロポニンのモニタリングや非侵襲的画像検査を行いながら心筋症の進展がないかを確認すること、また血栓症リスクのためのDダイマーやDVT発症の可能性を考えながら、抗凝固薬をふくめた適切な治療薬の選択が必要であると考えます。
こうやって見てみると、COVID-19の標的臓器の一つが心臓や血管であることは明らかです。我々循環器科医は対岸の火事として見るのではなく、様々な専門職と協力しながら、むしろ最前線に立つことが求められています。
参考文献
- escardio.org/Education/COVID-19-and-Cardiology/ESC-COVID-19-Guidance
- N Engl J Med. 2020 May 1;NEJMoa2007621
- JAMA Cardiol. 2020 Mar 25;e200950
- Circulation. 2020 May 19;141(20):1648-1655
- J Am Coll Cardiol. 2020 May 12;75(18):2352-2371
- N Engl J Med. 2020 May 1;NEJMoa2006923
- https://www.mhlw.go.jp/content/000631552.pdf
- Lancet. 2020 Mar 28;395(10229):1054-1062
- Circulation. 2020 May 18. doi: 10.1161
- J Am Coll Cardiol. 2020 May 5;S0735-1097(20)35218-9
弓野 大
Dai Yumino, MD, PhD
COVID-19 and Cardiovascular Diseases:Latest Updates
COVID-19 still remains as ferocious infectious disease around the world as of May 2020. As many COVID-19 related research been reported around the globe, the association between cardiovascular diseases and prognosis has gained attention. From our previous report >, we'd like to update on both COVID-19 and cardiovascular diseases through most updated reports.
COVID-19 and Cardiovascular Diseases
According to the European Society of Cardiology Guidance on COVID-19, presence of cardiovascular diseases is associated with increased risk of severe symptoms of COVID-19 and mortality*1. The association between the severity of COVID-19 and cardiovascular disease is starting to reveal. However, it is important to identify confounding bias as the age itself strongly affect the severity and mortality.
In addition, the guidance states on myocardial damage due to elevated troponin levels as a cardiovascular disease developed due COVID-19 infection. According to the latest Circulation review, myocardial damage is present in approximately one-quarter of COVID-19 infections which is caused by either acutely at the time of onset or progresses with progresses with deterioration of patient's condition*4.
COVID-19 and ACE Inhibitors/ARB
Both European and US guidance address the issues regarding COVID-19 and the renin-angiotensin enzyme, ACE2*1,5. The guidance recommends that discontinuation of ACE inhibitors / ARBs is a risk of exacerbation of the underlying disease and should be continue the medical therapy regardless of COVID-19 infection.
Consequently, there is currently no evidence to suggest that ACEIs or ARBs should be discontinued due to concern about COVID-19 infection. It is considered there may be more disadvantages of discontinuing the medical therapy.
COVID-19 and thrombotic complications
Thrombosis events such as stroke among young patients have been reported and the association between COVID-19 and thrombosis has drawn attention. It is known that severe infections and severe pneumonia are moderate risk factors for deep vein thrombosis (DVT). If the level of D-dimers elevates beyond the normal level, anticoagulation therapy, such as heparin, is recommended as COVID-19 patients may experience fibrinolytic system abnormalities due to cytokine storm and endovascular damage.
As we start to see the evidences around the association between COVID-19, anticoagulation therapy is recommended, however, we should remind ourselves that anticoagulation therapy could cause bleeding complication. For the usage of anticoagulants in COVID-19 patients, further guidance is awaited.
As we must co-exist with Corona virus, it is important to manage cardiovascular diseases on daily basis in order not to suffer from the virus. When we face a COVID-19 patient, we must consider the risk of secondary myocardial damage and check for the development of cardiomyopathy by monitoring troponin level or utilizing non-invasive imaging. Also, to prevent thrombotic event, the choice of medication including anticoagulants is critical and should follow D-dimers and consider for possibility of developing DVT
It is clear that one of the target organs of COVID-19 is the cardiovascular system. We, cardiologists, must cooperate with other medical professionals and lead this battle against COVID-19.
Reference:
- escardio.org/Education/COVID-19-and-Cardiology/ESC-COVID-19-Guidance
- N Engl J Med. 2020 May 1;NEJMoa2007621
- JAMA Cardiol. 2020 Mar 25;e200950
- Circulation. 2020 May 19;141(20):1648-1655
- J Am Coll Cardiol. 2020 May 12;75(18):2352-2371
- N Engl J Med. 2020 May 1;NEJMoa2006923
- https://www.mhlw.go.jp/content/000631552.pdf
- Lancet. 2020 Mar 28;395(10229):1054-1062
- Circulation. 2020 May 18. doi: 10.1161
- J Am Coll Cardiol. 2020 May 5;S0735-1097(20)35218-9
弓野 大
Dai Yumino, MD, PhD

