

新型コロナウイルス感染症(COVID-19)、ACE2、心血管系疾患の関係,Association of COVID-19, ACE2 and Cardiovascular Disease
当院の外来での出来事です。
76歳男性、高血圧性心疾患、慢性心不全のかかりつけの患者さん
「顔が赤い、熱っぽい、息切れもある、コロナからもしれないから診てくれ。」とひどい慌てた様子で連絡がありました。
2019年12月、湖北省武漢で発生した新型コロナウイルス感染症(COVID-19)は、急速に中国全土、ヨーロッパ、アメリカへと広がり、WHOは3月11日に「パンデミック(世界的な大流行)」を宣言しました。この2~3ヶ月の間に、新型コロナウイルス感染症の様々な研究報告がなされていますが、その中で、COVID-19の予後と心血管系疾患との関連性が注目されています(N Engl J Med 2020; 382:1268-1269, China CDC Weekly 2020; 2(8):113-122)。 今週には、COVID-19とRAAS阻害薬について、NEJMにて特集としてあげられています(N Engl J Med. 2020 Mar 30. doi: 10.1056/NEJMsr2005760)。
そこで今回のコラムは、新型コロナウイル感染症と心血管系疾患について取り上げたいと思います。
1. COVID-19における心血管疾患の合併は多い?
COVID-19に関するいくつかの論文が、早い段階から、高血圧症合併患者において、COVID-19が過剰に出現する可能性を注意喚起していました(Lancet Respir Med 2020 March 11)。実際に、中国における新型コロナウイルス感染症患者1,099人では、最も多い併存症は高血圧症であり、有病率は15%と報告されています(N Engl J Med. 2020 Feb 28. doi: 10.1056/NEJMoa2002032)。その他、中国における44,672人のCOVID-19 感染患者においては、4.2%は心血管系疾患、12.8%は高血圧症の既往があったとの報告がされています(China CDC Weekly 2020; 2(8):113-122)。また、単施設での99人(平均55.5歳・67%が男性)のCOVID-19感染者では、感染者の40%が心血管系疾患または脳血管疾患の既往があったという報告も上がっています(Lancet. 2020 Feb 15;395(10223):507-513)。さらに、入院患者138人の調査では、高血圧症が31%、糖尿病が10%、心血管疾患が14.5%、癌が7.2%であったとする報告もあります(JAMA. 2020 Feb 7. doi: 10.1001/jama.2020.1585)。このように、COVID-19における高血圧や心血管系疾患の割合は確かに多いように感じます。しかしながら、他の感染症における高血圧症の有病率のデータ(Ann Thorac Med. 2019 Jul-Sep;14(3):179-85)や中国における疫学調査(Lancet. 2017 Dec 9;390(10112):2549-2558)から、推定される高血圧の有病率と同じぐらいか、またはむしろ低い結果になっています。これらを総合すると、高血圧症や心血管系疾患が新型コロナウイル感染症で多いかは、いまだ統一した見解が出ていないのが現状です。つまり、高血圧や心血管系疾患をもっているとCOVID-19 にかかりやすいかどうかは、いまの段階では明らかではないと考えます。
2. COVID-19の重症患者に心血管疾患既往が多い?
中国の新型コロナウイルス感染症で死亡した113例の検討では、死亡群は回復した群の116例と比較し、高齢(年齢中央値:死亡群68歳・回復群51歳)で、高血圧症(死亡群48%・回復群24%)と心血管疾患(死亡群14%・回復群7%)の合併が多かったと報告されています。さらに、死亡例の77%に急性心筋障害、49%に心不全が合併しており、続発症としての心血管疾患にも注意を払わなくてはならないと考えます(BMJ. 2020 Mar 26;368:m1091. doi: 10.1136/bmj.m1091)。また、52人のICU管理となった新型コロナウイルス感染者の重症例の報告では、平均年齢が59.7歳で、観察期間28日において、死亡率は61.5%であり、心血管疾患合併は生存群で20%であったのに対して、死亡群で53%であり、心血管疾患の合併は予後を悪化させることも報告されています(Lancet Respir Med. 2020 Feb 24. pii: S2213-2600(20)30079-5)。PCR検査陽性191例の報告では、54人が死亡、137人が生存し、死亡オッズは年齢で上昇していましたが、死亡した患者は生存している患者に比べて合併症の罹患率が高く、高血圧症は死亡群48%・生存群23%、糖尿病は死亡群31%・生存群14%、冠動脈疾患は死亡群24%・生存群1%であったと報告されています(Lancet. 2020 Mar 28;395(10229):1054-1062)。その他、アメリカからは、COVID-19感染の重症者における心不全合併率は40%以上とかなり高いと報告が上がっています (JAMA. 2020 Mar 19. doi: 10.1001/jama.2020.4326)。これらより、COVID-19の予後不良因子には、心血管系疾患の合併が関わっていること、また続発性の急性心筋障害や心不全を発症するケースもあるため、注意して臨床経過をみていかなければならないことが分かります。なお、今回は、心血管系疾患に注目はしていますが、解析結果を眺めると、「高齢」という因子が最も強いこともあり、細かいことにはなりますが、独立した因子としての心血管系疾患がどこまで有意なものになるかは、更なる大規模な研究結果が必要と考えられます。
3. 新型コロナウイルス、アンギオテンシン変換酵素2(ACE2)、心血管疾患の関連性
新型コロナウイルスはACE2の膜蛋白作用を介して、細胞に侵入し感染することがわかっています(Trends Pharmacol Sci. 2004 Jun;25(6):291-4, Nat Rev Cardiol. 2020 Mar 5. doi: 10.1038/s41569-020-0360-5)。さらに、ウイルスが細胞内に感染するとACE2の発現が抑制され、肺損傷を起こす可能性も基礎研究で報告されています(Nat Med. 2005 Aug;11(8):875-9)。このACE2はヒトの血圧や循環を調整するレニン・アンギオテンシン(RAA)系においては、酵素として働き、高血圧症や心不全、糖尿病などに影響を与えています。ACE2は血圧を上昇させたり、炎症を引き起こしたりする作用のあるアンギオテンシンⅡをアンギオテンシン(1-7)に分解することが主な作用であり、生体において、圧負荷のようなストレスに暴露された際の適応に重要な役割を演じていたり、老化にも関わっていると考えられています。新型コロナウイルス感染症患者では、アンギオテンシンⅡが上昇しており、ウイルス量と肺損傷の重症度と相関していたという報告もあります(Sci China Life Sci. 2020;63(3):364-74)。新型コロナウイルス患者においてACE2が増加することが良いことかどうかは分かりません。つまりACE2が増えることにより肺の膜蛋白作用が増強され、よりウイルスを取り込みやすくする可能性があること、一方でRAAS系においてはアンジオテンシンIIを分解する酵素として働き、肺障害を抑制できる可能性があるからである。いずれにせよ、最近の研究報告からは、ACE2を介して、新型コロナウイルスと心血管疾患には強い関連性があることは見えてきたと考えます。新型コロナウイルス肺炎、心血管系疾患、そしてACE2の因果関係は、引き続き研究結果が待たれるところである。
4. 新型コロナウイルス感染症とアンギオテンシン変換酵素(ACE)阻害薬・アンギオテンシンⅡAT1受容体遮断薬(ARB)
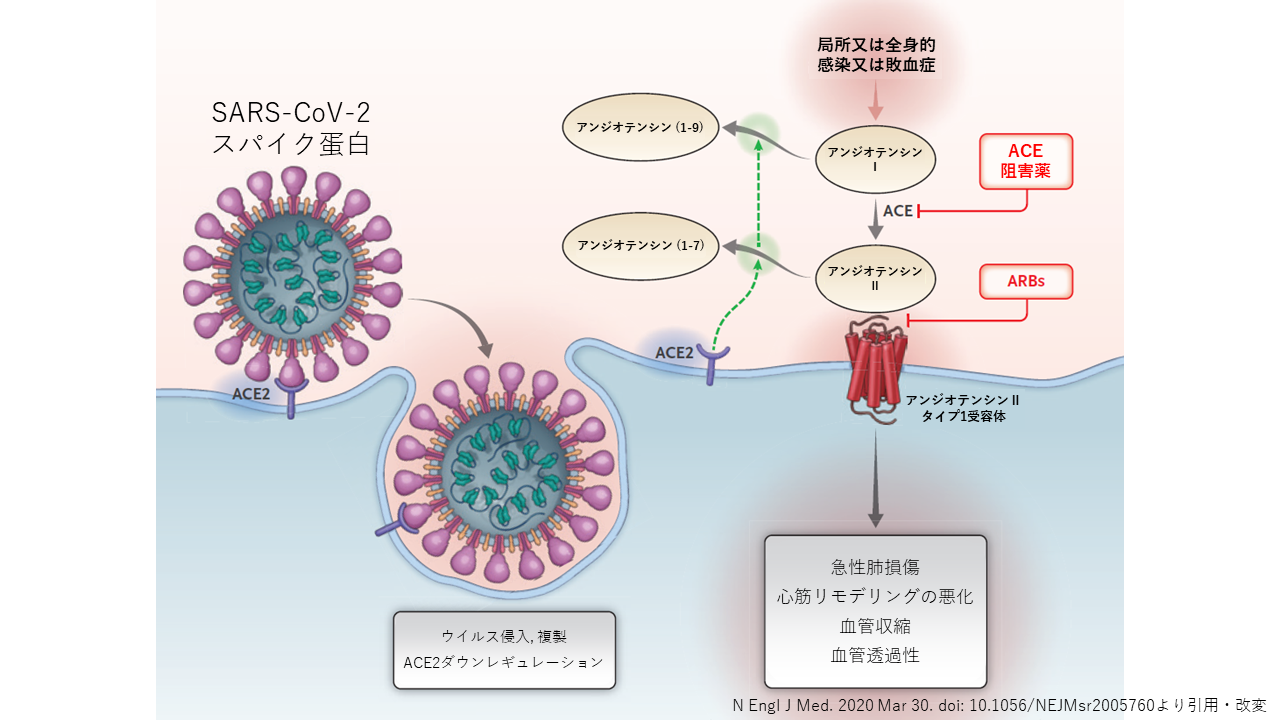
図は、最近のNEJMからの引用になります(N Engl J Med. 2020 Mar 30. doi: 10.1056/NEJMsr2005760)。SARS-CoV-2のウイルス細胞がACE2へ結合し、細胞内へ取り込まれ、またACE2はdown-regulateされアンジオテンシンIIの蓄積をもたらします。RAA系の活性は、ウイルス傷害に対する肺損傷反応を促進させる可能性をもちます。
高血圧症や慢性心不全、動脈硬化疾患の治療に使用するACE阻害薬やARBが、ACE2の発現を増加させる可能性がいくつかの動物モデルから報告されています。(Hypertension. 2020 Jan;75(1):173-82)。このCOVID-19が世界に広まり始めたときに、ACE阻害薬やARBを服薬していることが多い心血管系疾患をもつ患者に新型コロナウイルス感染症が多く、重症化しやすいのではないかという仮説がありました。一方で、ACE2は、肺損傷を引き起こす炎症促進作用のあるアンギオテンシンⅡを抑制することで、肺の炎症を抑える機序もあることが示されており、さらにACE阻害薬やARBにより炎症を抑えることも報告されています(Circulation. 2005 May 24;111(20):2605-10, N Engl J Med. 2020 Mar 17. doi: 10.1056/NEJMc2004973)。そのような中で、ACE阻害薬やARBの中止変更を検討するべきではないかという意見の論文も発表されました(Lancet Respir Med. 2020 Mar 11. pii: S2213-2600(20)30116-8)。これらの議論をうけて、ヨーロッパ心臓病学会は、新型コロナウイルスに関連してACE阻害薬およびARBの有害な効果を裏付ける証拠はなく、新型コロナ感染のためにACE阻害薬またはARBによる治療を中止することを示唆する臨床的または科学的証拠がないため、通常の降圧療法による治療を継続することを強く推奨するという声明を出しています(Position Statement of the ESC Council on Hypertension on ACE-Inhibitors and Angiotensin Receptor Blockers.)。また、アメリカ心臓協会(AHA)、アメリカ心不全学会(HFSA)、アメリカ心臓病学会(ACC)の3学会から「ACE阻害薬、ARBの服用は、新型コロナウイルス感染症罹患後の重症化要因にはならない」という共同声明も出ており、現時点では、ACE阻害薬、ARBを継続することが推奨されています(Patients taking ACE-i and ARBs who contract COVID-19 should continue treatment, unless otherwise advised by their physician.)。
冒頭の当院外来の慢性心不全患者さんの話に戻します。
「顔が赤い、熱っぽい、息切れもある、コロナからもしれないから診てくれ。」とのことで診察をしました。確かに顔はうっすらと赤くほてり、少し興奮した様子です。収縮期血圧は170と高く、脈拍も100とはやく、体温は36.2℃と平熱でした。呼吸は頻呼吸、呼吸音は正常でした。「コロナを毎日メディアで見ていてどんどん不安になる。それに加えて子供からは、"降圧剤を飲んでいるとまずいかもしれない"、と言われてさらに不安になり、降圧剤を自己中断してしまいました。」とのこと。しばらく傾聴すると、不安が解消されたのか、少しずつ硬かった表情が緩みはじめ、自然と血圧も下がり、呼吸状態も安定していきました。
新型コロナウイルス感染症とACE2、心血管系疾患の関係性があることを、これまでの研究報告からお示ししました。しかしながら、いまだ降圧剤や心不全治療薬となるACE阻害薬やARBを投与することにより、新型コロナウイルス感染症が「増悪するのか、改善するのか、また変わらないか」、は明らかにはなっていません。ただ、このようなウイルス感染症に罹患する可能性が高いなかで、今までよりもさらに循環器疾患のコントロールを厳格に行っていくことが大切であり、もしこれから感染患者を診ることがあれば、未だそれ自体の治療方法が確立していないなかで、致死的な合併症となりうる急性の循環器疾患、また心不全への罹患の可能性があることを念頭に置きながら診療にあたる必要性があると考えます。
さいごに
いま多くの人々が新型コロナウイルスに不安と恐怖を感じながら過ごしています。 わたしたち都心部にある心臓を専門とするクリニックとしてできることは、目の前の患者さんをしっかりと診ていくことともに、このようなコラムを通して、少しでも多くの患者さんが安心して過ごせるための一助になればと考えております。
いま世界中で蔓延している人類とウイルスとの未曾有の戦争が、少しでも早く落ち着き、人々がまた穏やかに住み慣れたところで過ごすことができることを切に願っております。
Association of COVID-19, ACE2 and Cardiovascular Disease
This is what happened at our outpatient clinic.
76 years old male patient with history of hypertension and chronic heart failure.
He called us claiming "my face is red, I am feeling hot, and suffering shortness of breath. I am concerned that I might be infected with COVID-19 and need you to come see me."
The novel coronavirus (COVID-19) emerged in Wuhan, China, in late 2019 and has quickly spread through China, Europe, and the United States. WHO made a remark on March 11th that the situation is "pandemic" significantly impacting the health of the world. Various researches on COVID-19 were reported in the past few months. Some of the researches report on the association of COVID-19 infection susceptibility and prognosis for patients with cardiovascular disease (N Engl J Med 2020; 382:1268-1269;China CDC Weekly. 2020;2:113-122). This week, there a special report in N Engl J Med focusing on COVID-19 and RAAS inhibitors (N Engl J Med. 2020 Mar 30. doi: 10.1056/NEJMsr2005760). In this article, I would like to focus on COVID-19 and cardiovascular diseases.
1.COVID-19 linked with more cardiovascular disease?
Several reports called the potential overrepresentation hypertension among COVID-19 patients from early on (Lancet Respir Med 2020 March 11). A report from China analyzing 1,099 patients reported that hypertension was the most common comorbidities with 15% prevalence rate (N Engl J Med. DOI: 10.1056/NEJMoa2002032). Even though the rate of hypertension and cardiovascular disease among COVID-19 patients varies, the epidemiological data indicate that the prevalence of hypertension is the same or rather less than other infectious diseases. Therefore, there is no consensus that COVID-19 is linked with more cardiovascular diseases as of today.
2.Patients with cardiovascular disease are at higher risk for developing COVID-19?
One report from China analyzing 113 who deceased and 161 who recovered with a diagnosis of COVID-19 shows that deceased patients were older (median age: 68 years vs 51 years), had more hypertension (48% vs 24%), and had more cardiovascular diseases (14% vs 7%). In addition, the author brings attention to common complications in deceased patients that 77% of them had acute cardiac injury and 49% had heart failure. This indicates that physicians need to pay closer attention to care and treat patients with cardiovascular disease(BMJ. 2020 Mar 26;368:m1091. doi: 10.1136/bmj.m1091). Another publication from the United States reported that more than 40% of patients with severe symptoms of COVID-19 had heart failure(JAMA. 2020 Mar 19. doi: 10.1001/jama.2020.4326). However, as the age being the highest risk factor, it is clear that a physician needs to pay close attention to the prognosis of cardiovascular comorbidity, acute cardiac injury, and heart failure.
3.Association of Coronavirus, Angiotensin-Converting Enzyme 2 (ACE2) and Cardiovascular Disease
The mechanism of how coronavirus enter the cells through ACE2 is known(Trends Pharmacol Sci. 2004 Jun;25(6):291-4, Nat Rev Cardiol. 2020 Mar 5. doi: 10.1038/s41569-020-0360-5). Once the virus is taken into the cell, ACE2 is further down-regulated and could mediate lung injury(Nat Med. 2005 Aug;11(8):875-9). There is a report that COVID-19 patients had elevated level of Angiotensin II and the viral loads correlated with the severity of lung injury (Sci China Life Sci. 2020;63(3):364-74). Though these findings are based on animal testing and basic research that it is not yet established for humans, we see that there is a strong association between coronavirus and cardiovascular disease with virus entry into cells through ACE2
4.COVID-19 and Angiotensin Converting Enzyme (ACE) Inhibitors and Angiotensin II AT1 Receptor Blockers (ARB)
The Figure is cited from the recent article from NEJM(N Engl J Med. 2020 Mar 30. doi: 10.1056/NEJMsr2005760). The figure shows interaction between SARS-CoV-2 and the Renin-Angiotensin-Aldosterone System leading to down-regulation of ACE2 resulting in angiotensin II accumulation. Activation of the renin-angiotensin-aldosterone system may mediate lung injury responses to viral. There are few animal research results reporting the increase of ACE2 level due to the usage of ACE inhibitors and ARBs which are commonly used in treating hypertension and chronic heart failure(Hypertension. 2020 Jan;75(1):173-82). When COVID-19 started to outbreak in the world, there was a hypothesis that patients with cardiovascular disease taking ACE inhibitors and ARBs may be more susceptible to the virus. In such situation, a publication recommending that patients should continue their ACE inhibitors and ARBs was published. Recently, the Council on Hypertension of the European Society of Cardiology strongly recommend that physicians and patients should continue treatment with their usual anti-hypertensive therapy"(Position Statement of the ESC Council on Hypertension on ACE-Inhibitors and Angiotensin Receptor Blockers). At the same time, Statement from the American Heart Association, the Heart Failure Society of America and the American College of Cardiology made a statement to "recommend continuation of angiotensin converting enzyme inhibitors (ACE-i) or angiotensin receptor blocker (ARB) medications for all patients already prescribed for indications" (Position Statement of the ESC Council on Hypertension on ACE-Inhibitors and Angiotensin Receptor Blockers).
Back to the story of one elderly patient with heart failure at the beginning
He called us claiming "my face is red, I am feeling hot, and suffering shortness of breath. I am concerned that I might be infected with COVID-19 and need you to come see me."
When we got to see him in person, his face was slightly red and he was rather in a little bit of panic. His systolic pressure was 170, his pulse was beating as fast as 100bpm, but his body temperature was normal with 36.2℃. He had Tachypnea, but the respiratory sound was normal. He said "I get more and more anxious everyday watching the news of COVID-19. Even my child told me that taking hypotensive medication may not be good for my health now. So, I stopped taking the medication." After listening his stories for a while, his anxiety seems to be resolved that his facial expression softened, blood pressure dropped, and respiration was stable.
This article showed the recent findings on the association between the novel coronavirus and ACE2 and cardiovascular disease. It is uncertain, as of today, that ACE inhibitors and ARBs may or may not impact the prognosis of COVID-19 infection. The only thing that is crystal clear is that the control of cardiovascular disease remains or even more critical in this situation. If physicians need to treat infected patients, we should keep in our mind that it is crucial to treat the patient to prevent acute cardiovascular injuries and develop heart failure as there is no cure for the infection for now.
Many people are living with worry and anxiety for the novel coronavirus. Our clinic, as heart specialists, will continue to do our best to support the patients and deliver health-related communications to provide the sense of safety and peace.
We sincerely hope this unprecedented war between human and virus will end very soon and get our peaceful daily life back.
弓野 大
Dai Yumino, MD, PhD

